2026-07-03
Melasma Series Part 2: Why is Melasma So Hard to Treat? (Evidence-Based Explanation)
Melasma is a complex condition involving changes in the entire skin environment, not just excess melanin. Discover why it is so difficult to treat and prone to relapse based on scientific research.
Not just a melanin problem, but a change in the entire skin environment
During melasma consultations at the dermatology clinic, there are questions I hear all the time.
‘Why is my melasma so hard to get rid of?’
‘Why does it come back even after laser treatments?’
It is easy to think of melasma simply as a state of excess pigment in the skin,
but recent studies view melasma not as a simple pigment disorder, but as a condition where the entire skin environment has changed.
In other words, melasma is a complex disease where not only melanocytes are overactivated, but also the
epidermis,
basement membrane,
upper dermis,
blood vessels,
inflammatory cells,
and fibroblasts
are all involved together.
This is why treatment is difficult, and why it often relapses even after improving.
Today, I will summarize why melasma is so hard to treat based on scientific papers.
1. Melasma is not a disease of just epidermal pigment
Generally, the treatment response of pigment disorders varies depending on which layer the pigment is located in.
Pigment confined to the epidermis usually responds relatively well to treatment,
but melasma is not that simple.
In melasma-prone skin, we observe:
Increased melanin across all layers of the epidermis
An increase in larger, more mature melanosomes
Melanin granules in the upper dermis
Increased melanophages in the dermis
all occurring simultaneously.
In short, melasma is not just a simple epidermal pigmentation,
but rather a condition involving changes in both the epidermis and the dermis.
Therefore, approaching it like a simple blemish that can be removed in one go has its limits.
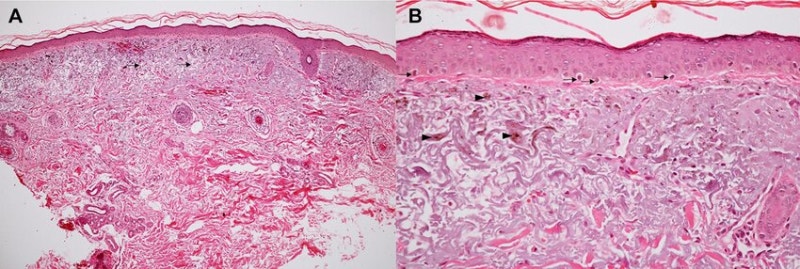
2. When the basement membrane is damaged, melasma goes deeper and lasts longer
Between the epidermis and the dermis, there is a structure called the basement membrane.
This basement membrane acts as a boundary for the skin, regulating the movement of melanin and various signaling molecules.
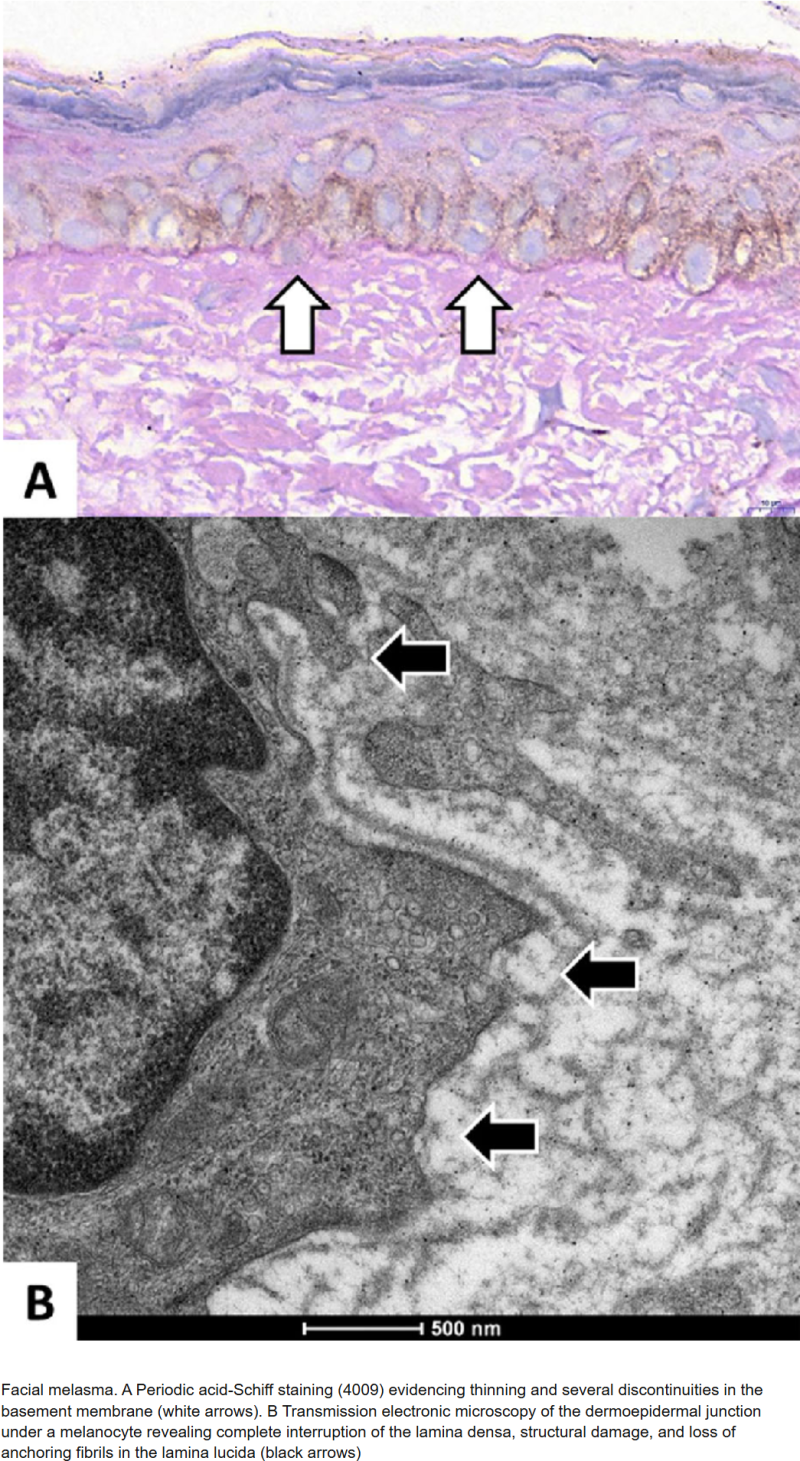
However, in melasma-affected skin,
increased discontinuity of the basement membrane,
thinning of the lamina densa,
and loss of anchoring fibrils
are commonly reported changes.
In other words, the basement membrane is in a damaged state.
When this happens, inflammatory and melanin-promoting signals rising from the dermis are more easily transmitted to the epidermis, and melanin-related changes can last much longer.
Ultimately, basement membrane damage is
one of the reasons why melasma deepens, easily relapses, and feels slow to respond to treatment.
3. Melasma is not just a disease of melanocytes
In the past, melasma was understood simply as a ‘disease where melanocytes overwork,’
but recently, a much more complex pathophysiology has been revealed.
In melasma skin, various cells surrounding the melanocytes
work together to stimulate melanin production.
The primary cells involved include:
Keratinocytes
Fibroblasts
Mast cells
and endothelial cells.
When these cells are exposed to UV rays and inflammatory stimuli, they secrete various growth factors and cytokines, resulting in continuous stimulation of the melanocytes.
Thus, melasma is not created by melanocytes alone, but by the surrounding skin environment working together.
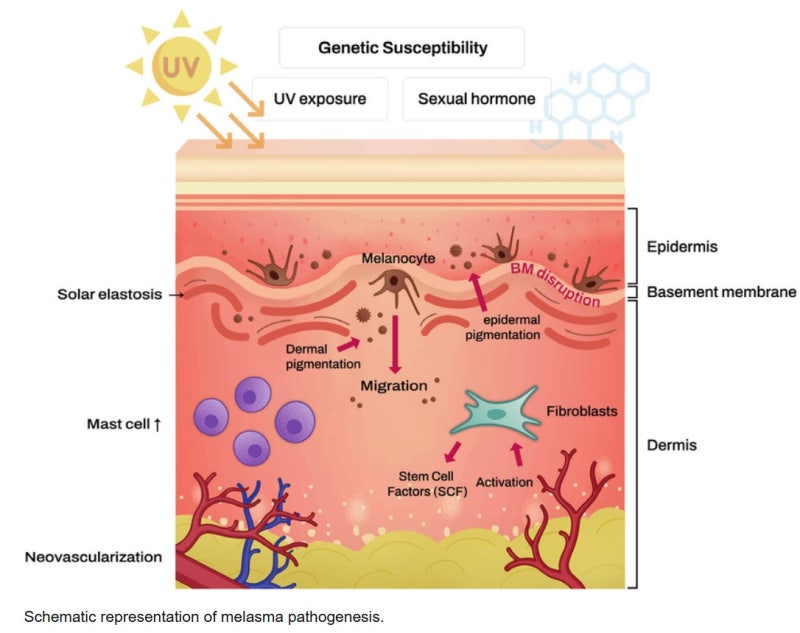
4. UV rays do not simply make melasma ‘darker’
The most important environmental factor in melasma is still ultraviolet (UV) radiation.
However, the role of UV rays goes far beyond just producing melanin.
According to research papers, UV rays can simultaneously cause:
Promotion of melanin production
Increased oxidative stress
Induction of inflammatory responses
Basement membrane damage
Changes in the upper dermis
and an increase in signals related to vascular proliferation.
In particular,
UVB has a major impact on the epidermis and basement membrane,
UVA affects deeper into the upper dermis,
and even blue-violet light within the visible spectrum can induce pigmentation in people with darker skin tones.
Therefore, melasma is not simply ‘getting darker from seeing too much sun,’
but a persistent condition where UV rays alter the structure and function of the entire skin.
5. Inflammation and oxidative stress keep melasma going
Melasma also has the characteristics of an inflammatory pigment disorder.
Factors such as UV rays, friction, irritating cosmetics, excessive procedures, and contact dermatitis
can create micro-inflammation in the skin,
and this inflammation, in turn, stimulates melanin production.
Additionally, oxidative stress plays a crucial role in melasma.
Studies report findings such as:
Decreased glutathione
Increased malondialdehyde
Increased nitric oxide
and an imbalance in the antioxidant system.
This means that melasma-prone skin is not just skin with a lot of pigment,
but a skin environment repeatedly exposed to inflammation and oxidative stimuli.
Therefore, melasma treatment should not just focus on removing pigment,
but must also move towards minimizing skin irritation and reducing inflammation and oxidative stress.
6. Fibroblast senescence can sustain melasma
One of the key concepts recently highlighted in the pathophysiology of melasma is
senescent fibroblasts (aging fibroblasts).
Senescent fibroblasts are not simply cells with declined function;
rather, they can secrete various melanin-promoting factors.
For example,
SCF,
HGF,
bFGF,
KGF,
and NGFβ
are among these substances.
These factors continuously stimulate melanocytes, creating an environment that sustains melasma.
In other words, melasma is not just an epidermal issue,
but a structure where the aged skin environment of the upper dermis continuously stimulates epidermal pigmentation.
7. Mast cells and blood vessels are also involved in melasma
In melasma skin, an increase in mast cells is observed,
and cases of increased vascular density are also reported.
Mast cells can secrete substances like
histamine,
tryptase,
and VEGF,
which are respectively involved in
promoting melanin production,
damaging the basement membrane,
vascular proliferation,
and altering the dermal structure
as contributing factors.
Skin with increased blood vessels goes beyond just looking red;
it can also be linked to an environment that stimulates melanocytes.
Therefore, some forms of melasma
must be understood as having vascular and inflammatory components alongside the pigmentation.
8. Melasma becomes more sensitive when the skin barrier is weakened
There are also reports that melasma skin may have slower skin barrier recovery compared to normal skin.
The stratum corneum is thinner, barrier recovery after irritation is delayed,
and the skin can react more sensitively to external stimuli.
For this type of skin,
excessive exfoliation,
frequent peeling,
strong lasers,
rubbing habits,
and irritating cosmetics
can all become aggravating factors.
In other words, what is important in melasma treatment is not unconditionally treating it aggressively,
but managing it stably while protecting the skin barrier.
9. This is why melasma frequently relapses
The reason melasma relapses so easily is clear.
Melasma is not a condition that ends simply by erasing the pigment left on the skin;
it is because the environment that recreates that pigment still remains.
In melasma skin,
UV sensitivity,
inflammatory responses,
oxidative stress,
basement membrane damage,
upper dermal changes,
increased blood vessels,
senescent fibroblasts,
and mast cell activation
can all coexist.
Therefore, even after treatment,
if influenced by sunlight, heat, irritation, hormonal changes, dermatitis, or lifestyle habits,
it is easy for it to flare up again.
Summary
Melasma is not simply a disease of excess melanin.
In melasma skin,
Melanocyte overactivation
Increased UV response
Inflammation
Oxidative stress
Basement membrane damage
Vascular changes
Fibroblast senescence
Skin barrier abnormalities
all appear together.
Thus, melasma treatment is not just about extracting pigment,
but it is crucial to address the skin environment itself that continuously produces melanin.
Preview of the Next Part
In the next article,
I will summarize how we should actually approach melasma treatment.
How to properly use sun protection
What role topical medications play
When tranexamic acid is helpful
Where laser toning stands as a treatment
And why barrier management and minimizing irritation are important
will all be explained based on scientific papers.